Health Library
Familial adenomatous polyposis
You must carefully read the "Consumer Information Use and Disclaimer" below in order to understand and correctly use this information
What is familial adenomatous polyposis?
Familial adenomatous polyposis, or "FAP," is a disease that causes abnormal growths called "polyps" to form in the large intestine (the colon), rectum, and other areas (figure 1). The polyps are not cancer, but they can turn into cancer.
Most people with FAP have hundreds or thousands of polyps. So they have a much higher risk of getting colon cancer than other people. Without treatment, almost all people who have classic FAP get colon cancer by age 39 years. Some people have a milder form of FAP that causes fewer polyps (less than 100). In these people, cancer can develop later in life (in their 50s).
People with FAP can also get cancer of the stomach, small intestine, thyroid, pancreas, or brain.
FAP is caused by an abnormal gene that often runs in families. But some people have the abnormal gene even though no one else in their family had polyps or cancer.
People who have FAP usually start having symptoms in their teens or 20s. But some get it in childhood.
What are the symptoms of FAP?
FAP usually does not cause any symptoms unless cancer develops. Symptoms of colon cancer can include:
Bright red blood in bowel movements
Diarrhea (runny, watery bowel movements)
Constipation (trouble having bowel movements)
Belly cramps
Weight loss without trying
Bloating (feeling like the belly is full all the time)
Feeling tired
If someone in your family has FAP, your doctor might recommend you get a genetic test to check if you have it. The test might find FAP before you have symptoms.
Will I need tests?
Yes. Your doctor or nurse will ask about any symptoms and do an exam.
You might also have these tests:
Colonoscopy (figure 2) – The doctor puts a thin tube with a camera on the end into your anus and up into your colon to look for polyps or other problems. They can also take tissue samples. Then, another doctor looks at the samples under a microscope.
Sigmoidoscopy (figure 3) – This is very similar to a colonoscopy, but it only looks at the last part of your colon, close to your rectum.
Upper endoscopy (figure 4) – The doctor puts a thin tube with a camera on the end into your mouth and down into your esophagus and stomach to look for problems. They can also take tissue samples. Then, another doctor looks at the samples under a microscope.
Genetic testing – This is a blood test to look for the abnormal gene that causes FAP. Before the test, you will talk with a "genetic counselor." They can help you understand what having the gene could mean for you and your family.
You might have these tests in a different order or more than once. For example, if someone in your family has FAP, you might have genetic testing to see if you have the abnormal gene. Or you might have a colonoscopy to look for polyps. If a genetic test shows you have FAP, you might have a colonoscopy, or sigmoidoscopy and upper endoscopy. The tests can show your doctor how many polyps you have and where they are.
If you have FAP, your doctor might do exams or tests to look for other types of cancer, such as thyroid cancer.
How is FAP treated?
Treatment depends on your situation. Treatments include:
Colectomy – This is surgery to remove the colon, which also removes the polyps. This lowers your risk of getting cancer. It is the main treatment for FAP.
Removing the polyps – If you have a milder form of FAP that causes fewer polyps, your doctor might be able to just remove the polyps instead of doing a colectomy. They will remove the polyps during a colonoscopy or endoscopy.
Your doctor will talk with you about your treatment options and how to best lower your chances of getting cancer.
Images
figure 1: Colon and rectum
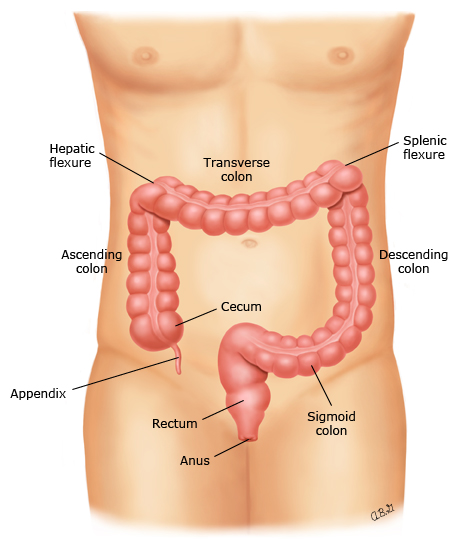
This figure shows the the colon (also known as the large intestine), the rectum, and the anus. Doctors use different names for different parts of the colon.
Graphic 58531 Version 10.0
figure 2: Colonoscopy
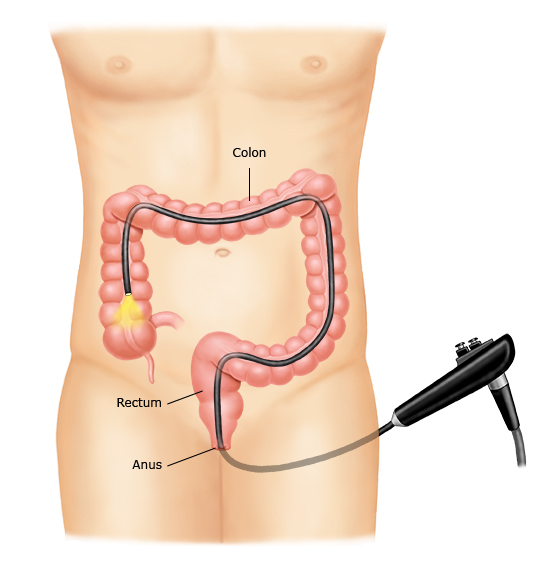
During a colonoscopy, you lie on your side or back and the doctor puts a thin tube with a camera into your anus (from behind). Then, the doctor advances the tube into the rectum and colon. The camera sends pictures from inside your colon to a screen.
Graphic 52258 Version 9.0
figure 3: Sigmoidoscopy
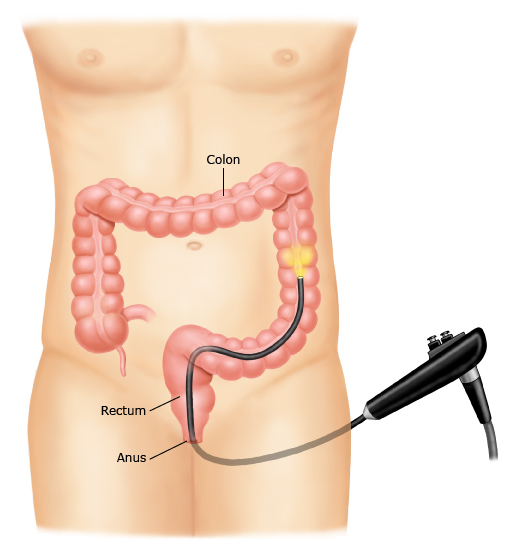
Duringa sigmoidoscopy, you lie on your side and the doctor puts a thin tube with acamera into your anus (from behind). Then, they advance the tube into your rectum and the last part of your colon. The camera sends pictures frominside your colon to a TV screen.
Graphic 143975 Version 1.0
figure 4: Upper endoscopy
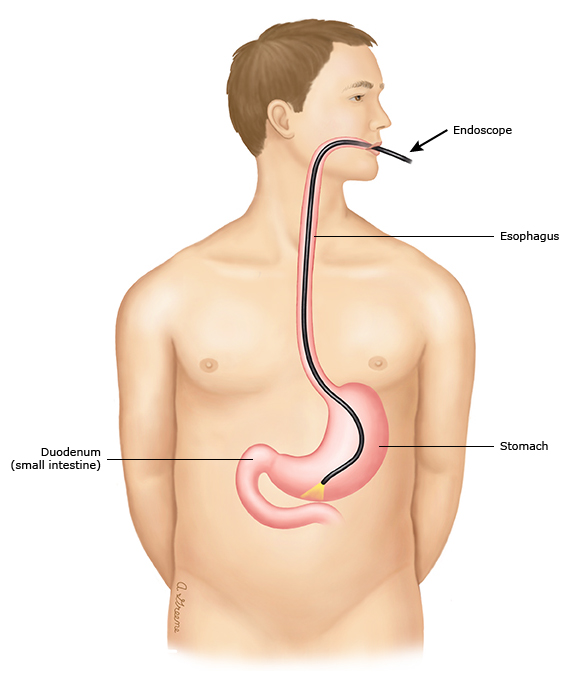
During an upper endoscopy, you lie down and the doctor puts a thin tube with a camera and light on the end (called an endoscope) into your mouth and down into your esophagus, stomach, and duodenum (the first part of your small intestine). The camera sends pictures from inside your body to a screen. That way, your doctor can see the inside of your esophagus, stomach, and duodenum.
Graphic 75392 Version 5.0
Give to a Healthier Future
Help us elevate and expand our care, make breakthroughs in biomedical science and improve community health and wellness.
Healthier communities. Healthiest lives. Together.